Labral tears in Rock Climbers
Two case reports
Marie-Claire Haddock
Medical student, The University of
Manchester
Lennard Funk Bsc. MSc. FRCS (Tr & Orth)
Department of
Orthopaedics, Hope Hospital.
Correspondence to: Mr Funk, Department of Orthopaedics, Hope Hospital, Stott Lane, Salford, M6 8HD, UK. Tel: +441612065169. Fax: +442061205. Len.Funk@srht.nhs.uk
Keywords: Rock climbing, SLAP lesions
Introduction
Rock climbing is one of the fastest growing sports in the world.1,2,3,4 Current data from the British Mountaineering Council suggest that there are approximately 150,000 active climbers in the UK.4 Historically, climbing injuries were primarily associated with acute trauma sustained from falls.1,2,3 The combination of an increased number of climbers and increased safety has led to more climbers with complex over-use injuries presenting to the medical profession.1,2,3 Current figures suggest that 65% of climbing injuries are over-use injuries; 90% of which affect the upper limb.1,2 Hand injuries account for 60% of these injuries. The remainder are divided almost equally between the elbow and the shoulder.1,2,3 The inherent instability of the shoulder puts it at great risk of injury during climbing as the forces and stresses applied to the joint are so different from those of normal activity.1,2
SLAP lesions, tears of the superior glenoid labrum that extend anteriorly to posteriorly,5,6 have been described in throwing athletes and gymnasts, but to our knowledge this is an undocumented injury in rock climbers.1,2,3,5,6,7 We present two case reports of SLAP lesions in such athletes. Both climbers presented with pain arising from the posterior aspect of the shoulder that was associated with painful clicking and exacerbated by overhead activity, typical of SLAP lesions.5,7 Interestingly, although both proved to have SLAP lesions their mechanism of injury and onset of symptoms were distinct. Although uncommon, these lesions can cause considerable disability.5,6,7 Excellent results can be achieved by arthroscopic repair.5,6
Concurrent shoulder pathology (such as rotator cuff tears; Bankart lesions; glenohumeral chondromalacia and anterior instability) are often found in patients ultimately proven to have SLAP lesions.5,6, The signs of which may mask those of the SLAP lesion resulting in misdiagnosis of primary impingement syndrome or biceps tendonitis.5,6,7 A high level of clinical suspicion is therefore needed for the correct diagnosis of SLAP lesion to be made.5,6,7 Standard radiographs should be taken to exclude other causes.5 Contrast magnetic resonance (MR) arthrogram with gadolinium is the imaging modality of choice with a sensitivity and specificity quoted at 89% and 91%, respectively, for SLAP lesions.8 This can also be used to aid their classification.5,8 Definitive diagnosis, lesion classification and repair are performed arthroscopically.5,6,7,8,9,10
Physical examination including the O’Brien’s test and the Kibler’s crank test is recommended.5The O’Brien’s test is quoted to have a sensitivity of 100% and a specificity of 98.5% for the diagnosis of Labral abnormailities.9 Kibler’s test is quoted as having a sensitivity of 84% and a specificity of 91.5% for diagnosing SLAP lesions.10 However, other papers have quoted much lower values than these and it is recognised that the diagnosis of SLAP lesions on clinical examination alone is limited.5,7
In O’Brien’s test, the patient's shoulder is held in 90° of forward flexion, 30–45° of horizontal adduction and maximal internal rotation. The examiner, holding the patient's wrist, resists the patient's attempt to horizontally adduct and forward flex the shoulder. The test is positive if this reproduces the patient’s pain. In the Kibler’s crank test, the patient's shoulder is abducted to 90° and slowly internally rotated while a gentle axial load is applied through the glenohumeral joint. The test is considered positive if the patient reports pain, catching, or grinding in the shoulder.
Patients and Methods
 Case report
1
Case report
1
A 22-year-old, right-handed student teacher presented with a 3-month history of pain arising from the posterior aspect of his left shoulder, this was associated with an audible click and exacerbated by overhead activity. The patient was a keen boulderer (see Appendix). Three months previously, he lost his footing while climbing and had to support his body weight by his arms. As his feet slipped, he heard and felt a loud, painful click in the left shoulder. Although painful, he continued to climb. However, on returning home the pain had worsened and he had not climbed since. He had tried physiotherapy, including ultrasound therapy, but did not find relief from his symptoms.
Clinically, he had full active range of movement with no scapula dysrhythmia. A visible and palpable clicking was present at 160° of abduction; this clicking reproduced his posterior shoulder pain. Kibler’s clunk test reproduced this pain and O’Brien’s test was positive. No other abnormalities were detected.
The MR arthogram showed a high signal within the anterior labrum extending towards the superior aspect of the joint with separation of the superior aspect. The tear did not continue posteriorly.
At arthroscopy the left shoulder a type III lesion was diagnosed and the superior labrum re-attached using two suture anchors. The anchors’ stability was confirmed by probing. No other abnormalities were seen.
Case report
2
A 58-year-old teacher presented with pain arising from the posterior aspect of her right shoulder. This was associated with painful clicking during overhead activity. She was a rock climber. There was no single traumatic event that precipitated her pain but she described an insidious onset of pain over 12 months. At the time of presentation, she was having great difficulties climbing and avoided putting her arm behind her back as this caused her pain.
Clinically, she had similar findings to the previous case: full range of movement; mild scapula dysrhythmia and a posterior-superior glenohumeral click which reproduced her pain. O’Brien’s test was strongly positive as was Kibler’s crank test.
The MR arthrogram suggested a type II tear from the 10 o’clock to 4 o’clock positions. The posterior labrum and the long head of the biceps’ tendon were intact.
At arthroscopy, a type II SLAP lesion was diagnosed. The SLAP lesion was repaired and the labrum and glenoid fixed with two suture anchors.
![]() Postoperative
management
Postoperative
management
In both cases, a sling was used postoperatively and gentle pendular exercises of the elbow, wrist and hand were prescribed. At 4–5 weeks’ postoperatively, active biceps strengthening was initiated and both patients were advised not to climb for 3 months. At 6-month review, both climbers made full recoveries and have returned to their previous climbing levels.
Discussion
Traction and compression are the most common mechanisms of SLAP lesions. Traction injuries result from a sudden pull in the inferior, anterior or superior direction.6,7,8 The latter commonly occurs when climbing overhanging walls when the climber loses foot contact with the wall and is forced to support his full body weight by his arms. During the dynamic move, common in sport climbing and bouldering (see Appendix), the climber (as quickly and forcibly as possible) pushes down against the first hold to launch himself to the next hold often reaching it with the arm fully extended and the shoulder abducted and externally rotated. On catching the next hold, it seems likely that much of his weight will suddenly be transmitted via the biceps tendon to the labrum before he places his feet.
Elite climbers train on campus boards (Fig. 1), with which they perform a series of repetitive, explosive pull ups to ‘jump’ between thin bars of wood, ascending like a ladder, so as to improve dynamic strength and accuracy. This activity could similarly result in sudden, extreme loading of the biceps’ anchor and subsequent tear of the labrum.6,7
In a fall the lead climber (see Appendix) outstretches, slightly abducts and forwardly flexes the arms; and hold their legs outstretched in front of them, slightly flexed at the knee and hip to absorb the impact with the rock face. This may result in a SLAP lesion from the combined compression of the biceps’ tendon and labrum between the glenoid fossa and the humeral head on impact.6,7 Further application of these forces may result in rotator cuff tear.5 If the arm were externally rotated on impact, the impact would cause the tear to propagate anteriorly. Alternatively, strong reflex contraction of the biceps or rotator cuff muscles may worsen the tear.5
A fall could result in a direct blow to the shoulder, this can cause a SLAP tear.5,6,7 Alternatively, patients may present with an insidious onset of shoulder pain with painful clicking, in the absence of a clear history of trauma. This presentation is seen in a third of patients who are ultimately proven to have SLAP tears.7 The repetitive, eccentric loading of the superior labrum and the biceps tendon insertion with the arm in external rotation and abduction (Fig. 2) is common in all climbing. It is the authors’ opinion that this repetitive stressing of the labrum may result in a SLAP tear of insidious onset. Cadaveric studies which simulated contraction of the long head of the biceps produced a strain on the anterior-superior and posterior-superior aspects of the glenoid labrum that was proportional to the load placed on the tendon.6 In addition, it was shown that this strain was significantly greater when the shoulder was abducted.6 This supports the hypothesis that prolonged strain of the labrum, with the shoulder weight bearing in this position, as commonly occurs when climbing, predisposes to the development of a SLAP tear.
Conclusions
Climbing itself predisposes people to developing SLAP tears due to the forces applied to the labrum during climbing and training. We would, therefore, like to emphasize that, due to the difficulties in making the diagnosis, medical practitioners should have a high index of suspicion of SLAP lesions in climbers presenting with a history compatible with SLAP lesion. A full physical examination of the shoulder, including O’Brien’s test and the Kibler’s crank test, should then be performed. Concurrent pathologies are common and should be tested for during the assessment.5,6,7 The imaging method of choice for those suspected clinically of having a SLAP lesion is MR arthrography with gadolinium.8 Those with clinical and radiological features of SLAP lesions should be arthroscoped for definitive diagnosis and/or arthroscopic repair of the lesion.5,6,7,8,9,10
![]()
Figure and Legends
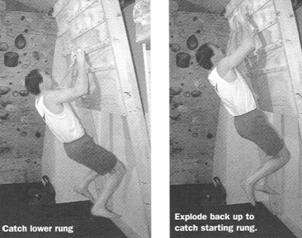
Figure 1. Dynamic campus board training. From How to Climb 5.12 by Hörst E, Guilford: Falcon Guide, a division of Globe Pequot. Copyright © 1997, 2003 by Eric J Hörst. Used with permission of The Globe Pequot Press, Guilford, CT, USA.
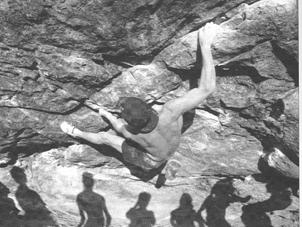
Figure 2. Eccentric loading of the biceps’ tendon with shoulder in external rotation and abduction. From Better Bouldering by J Sherman, Copyright © 1997 by John Sherman. Used with permission of The Globe Pequot Press, Guilford, CT , USA.
![]()
Appendix– Glossary of climbing terms
Bouldering
Climbing without ropes to a height from which you should be able to fall/jump and not hurt yourself (3 m). These routes are very short but often involve powerful, and sometimes dynamic, movements. A specially designed crash-mat is used to soften the landing. A boulderer, is a climber dedicated to this style of climbing.
Sport climbing
This is climbing in which the routes all have pre-placed stainless steel bolts either drilled in or chemically glued to the rockface. The most difficult sport climbs are often overhanging. This style of climbing, in particular, places great demands on the shoulders which quite literally play a pivotal role. On overhanging routes, the climber will fix one shoulder and arm (“lock off”) and use that as a pivot around which they will adjust the rest of the body using the truncal musculature.
The inherent safety of this type of climbing appeals to many people and due to the reduced fear of falling, many attempts can be made at hard moves. A corollary is that it is associated with more over-use injuries.1,2,3
Leading
This is what the first ‘active’ climber is doing as he/she climbs while placing the protection in traditional climbing or clipping the bolts in sport climbing, while the second ‘inactive’ climber is belaying the first.
![]()
References.
1. Haas J & Meyers M. Injury clinic: Rock climbing Injuries. Sports Medicine. 20 (3); 199-205.
2. Binney D. Clinical: Getting a grip of rock climbing injuries. Sport & Medicine Today. 2001; (Autumn): 199-205. Available at http://www.thebmc.co.uk/safety/hp/hprg_index.htm.%20Accessed%20October%206, 2005.
3. Rooks M. Rock climbing injuries. Sports Med. 1997; 23: 261–270.
4. The British Mountaineering Council website. Available at: http://www.thebmc.com/. Accessed January 10, 2005.
5. Snyder S. Superior Labrum anterior to posterior lesions of the shoulder. In: Shoulder Arthroscopy, 2nd edn. Philadelphia: Lippincott Williams & Wilkins; 2003: 147–166.
6. Grauer J, Paulos L, Smutz W. Biceps tendon and superior labral injuries. Arthroscopy. 1992; 8: 488–497.
7. Snyder S, Karzel R, Del Pizzo W, Ferkel R, Friedman M. SLAP lesions of the shoulder. Arthroscopy. 1990; 6: 274–279.
8. Bencardino J, Beltram J, Rosenberg Z, Rokito A, Schmahmann s, Mota J et al. Superior labrum Anterior- Posterior Lesions: Diagnosis with MR arthrography of the shoulder. Radiology 2000; 214: 267-271.
9. O’Brien S, Pagnani M, Fealy S, McGlynn S & Wilson J. The active compression test, a new and effective test for diagnosisng labral tears and acromioclavicular joint abnormaility. Am J Sports Medicine. 1998; 26:610-613.
10. Kibler W. Specificity & sensitivity of the anterior slide test in throwing athletes with superior glenoid labral tears. Arthroscopy. 1995; 11: 296-300.